One of the sure signs of an authoritarian regime is a passion to censor unwanted information, research, ideas, and history. The Trump administration is busy deleting scientific research at the Centers for Disease Control. Any studies that include data about LGBT+ people, women, or others whose existence is anathema to Trump and his Merry Band of Bigots is being purged. During the first Trump term, research about climate change was given the heave-ho, and scientists rushed to archive their work. Again, climate change is being buried in the archives of the EPA. Now the new Enemy of the State is DEI.
The Washington Post wrote about the censorship at the CDC here:
The Centers for Disease Control and Prevention removed or edited references to transgender people, gender identity and equity from its website Friday, racing to meet a late-afternoon deadline imposed by the federal Office of Personnel Management.
Whole pages about HIV testing for transgender people, guidelines for use of HIV medication and information on supporting LGBTQ+ youth health were no longer available late Friday.
The material removed or edited includes extensive sets of data collected and used by researchers around the world, according to two employees who spoke on the condition of anonymity out of fear of retaliation. The data’s removal will have implications for researchers who have relied for decades on the comprehensive material collected by the vaunted public health agency.
One example of a set of data taken down was a survey by the Youth Risk Behavior Surveillance System, conducted every two years to assess the health behaviors of high school students. The landing page for data about the survey was dark Friday afternoon and read: “The page you’re looking for was not found…”
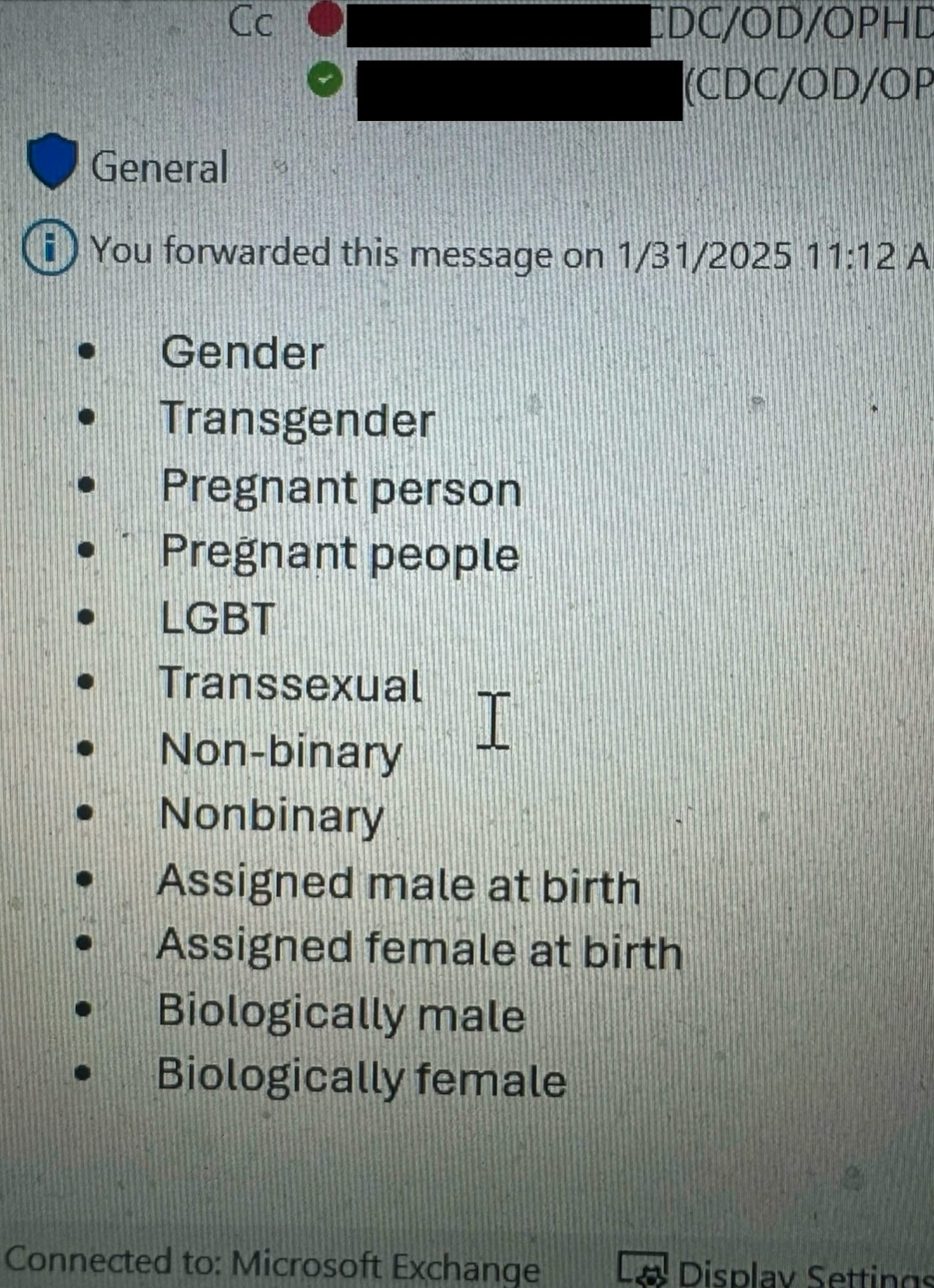
Agency staff members were given a list of about 20 words and phrases to be used as a “guide,” according to a screenshot shared by one employee. The words include: gender, transgender, pregnant person, pregnant people, LGBT, transsexual, nonbinary, assigned male at birth, biologically male, biologically female, he/she/they/them. All references to DEI and inclusion are also to be removed.
The new regime is moving fast to obliterate inconvenient science writes TCinLA at his Substack blog, which is called “That’s Another Fine Mess.”
There is a scene toward the end of Act Two in “Rollerball” (the first release, starring James Caan, the one worth watching) in which “Jonathan E” is allowed to go to Geneva, where the computer that runs the world is housed, to ask questions of it. He finds that the computer is systematically “losing” history and data. The Librarian tells him that “He’s already lost the entire Twelfth Century.” Jonathan E realizes that there will never be a way to rebel against the corporate overlords who run the world in which he lives, because the people will never know any other alternative.
Or as George Orwell put it in “1984″: “Who controls the past, controls the future; who controls the present, controls the past.” In that novel – which it seems some people are adapting now as a user’s manual – the information Big Brother’s government didn’t want people to access ended up in “the memory hole.”
As bad as we thought things would be with the second coming of Cletus J. Dumbass’s Maladministration, the reality is far worse. We are only at day 12 of this maladministration, and the assault on historical knowledge and information is well underway.
The Theocrats who created Project 2025 know what Orwell knew, what the screenwriter of Rollerball knew, what those who study authoritarian movements know: if people do not have access to information, they have no way to separate lies from truth. They can then be ruled without fear of revolt.
Information at the Centers for Disease Control is disappearing as you read this. The agency has already removed all scientific data from public view.
On Thursday night, word began to spread through the scientific community that researchers should go to the CDC website and download their data immediately, because such data was about to disappear from the website, or be altered to comply with Maladministration II’s ongoing plan to remove from federal agencies any mention of gender, DEI, or accessibility. Scientists were up throughout the night, working to download information they needed for their continued work on such crucial issues as tracking viral outbreaks. (Remember back in 2020, at the outbreak of the pandemic, when Cletus said he wished they would stop testing people and reporting the results because “It doesn’t look so good for me”?)
Already, the data from the CDC’s Youth Risk Behavior Surveillance System has disappeared. The data from the Agency for Toxic Substances and the Disease Registry’s Social Vulnerability Index and the Environmental Justice Index are gone. The landing page for HIV data has vanished. The AtlasPlus tool, which holds 20 years of CDC surveillance data on HIV, hepatitis, sexually transmitted infections, and tuberculosis, is no longer available. The new “leaders” at the CDC have directed employees to scrub any mention of “gender” from the data it shares at the website, replacing it with “sex.”
The purge’s full scope is still unclear. The Atlantic obtained a document that revealed the government – as of Thursday evening – planned to target and replace several “suggested keywords” – including “pregnant people,” “transgender,” “binary,” “non-binary,” “gender,” “assigned at birth,” “cisgender,” “queer,” “gender identity,” “gender minority,” and “anything with pronouns” These terms represent demographic variables researchers collect when tracking the ebb and flow of diseases and health conditions across populations. If they are reworded, or even removed entirely from data sets to comply with the Executive Order issued the night of Enshittification Day, researchers and health-care providers will have a much harder time figuring out how diseases affect specific communities.
The legislative “explicit purpose” of CDC data is to guide researchers to places and people who most need attention. It is hard to understand how this decision benefits health, but it does benefit an ideological decision to delete the entire topic of transgender.
When questioned about this today, an HHS spokesperson said that “all changes to the HHS website and HHS division websites are in accordance with President Trump’s January 20 Executive Orders” on gender and DEI.
The government understands these changes could have scientific implications since the document directing a review of CDC content suggests some work could be altered without “changing the meaning or scientific integrity of the content;” any such changes should be considered “routine.” Changing other content, would require review by an expert since any alterations would risk scientific integrity.
However, the document does not specify how data would be sorted into the two categories, or who would make such decisions.
The fear among researchers is that entire data sets could be taken down, reappearing with demographic variables removed or altered to conform with the DEI restrictions, losing entire sections of data. Since the Executive Order defines sex as binary, this means transgender people and nonbinary people could be erased. Such data could include facts such as gay men have higher rates of STIs, but lower rates of obesity and that transgender women have higher rates of HIV, but lower rates of prostate cancer, or how various demographic subsets of Americans are most at risk from conditions including adolescent depression, STIs, and sex-specific cancers
At this time, groups of researchers are rushing to archive the CDC website in full.
An example of what is at stake: Mpox – popularly known as “Monkey Pox” – affects people differently, with men who have sex with men being the primary group likely to be infected with the disease. Possessing that knowledge allowed medical authorities to more efficiently allocate resources, including vaccines, bringing the epidemic under control before it affected Americans more widely.
Scrubbing data such as this would change how the government allocates funds for long-standing threats to public health; this will widen health-equity gaps, or reverse progress in combating such diseases. The rates of STIs have recently started to plateau in the U.S., after decades of steady increase. Altering data that focus interventions on transgender populations, or men who have sex with men, would undo those gains. If there is no data to prove a health issue is concentrated in a particular community, that gives the government justification to cut funding.
Since much of the data on the CDC website comes from states, once it becomes known this data-scrubbing is happening, some states (blue states) may become reluctant to share information with the federal government while other states (red states) might not collect that important information at all. This would make what information the government does have unreliable, creating a skewed picture of reality.
It is shocking to realize how Project 2025 amounts to a war against modern society. Those reading this who are older than 75 can remember what life was like without the polio vaccine, without the measles and mumps vaccines. I escaped polio, but I came down with both measles and mumps before age 5, and I can still remember how difficult dealing with those was. The only thing I can compare those events to was coming down with COVID two years ago, which I survived only because I immediately obtained Paclovid for early treatment. Knowing to do that was because information about the disease and its effect on older people was made public by the CDC. Without that information, I and a lot of other older people who came down with COVID then would literally not be here now.
Maladministration II has to be seen as the all-out attack on modern society that it is. It has to be opposed by all means available. These Enemies of America are a minority. Every poll shows that significant majorities – over 66% – of Americans oppose every single action Project 2025 plans to take in this assault.
I admit that in my wildest nightmares of this coming to pass, I didn’t think of such things as an all-out attack on modern science, as is happening now. But this clearly demonstrates the nature of the threat we face. They are The Enemy. In all things, in all ways.
Winston Churchill warned his people in a speech given on June 18, 1940 that they were threatened by “a new Dark Age made more sinister, and perhaps more protracted, by the lights of perverted science.” We actually face that situation now.
The one fortunate thing is that, so far, the enemy has proven themselves largely incompetent to carry out successfully their plans to destroy modern civilization. That doesn’t make them less dangerous, but we can resist them.
We have to.